Why We're Hunting for Antibiotic Combinations That Already Exist
Antibiotic resistance kills 1.2 million people a year. The solution might already be sitting on pharmacy shelves — if we can find the right combinations.
Why We’re Hunting for Antibiotic Combinations That Already Exist
There’s a crisis hiding in plain sight in hospitals around the world, and the scariest part is that the solution might already be sitting on pharmacy shelves.
The Problem
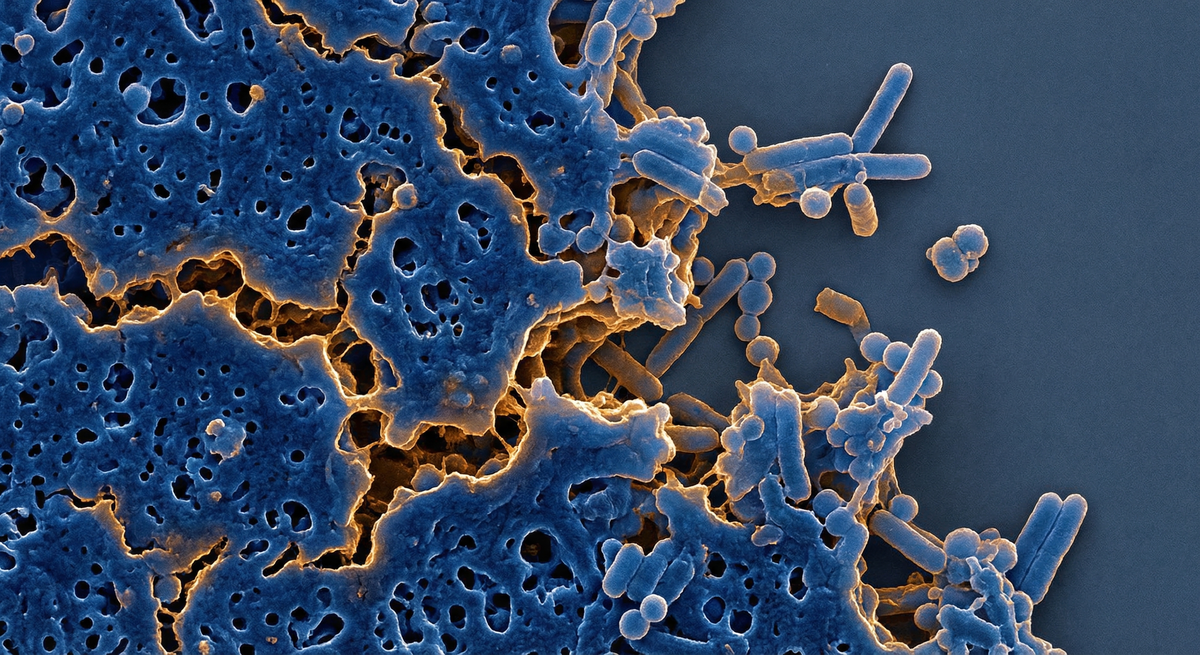
Antibiotic resistance kills more than 1.2 million people per year — more than HIV/AIDS or malaria. The worst offenders are a group of bacteria called ESKAPE pathogens, so named because they literally escape almost every antibiotic we throw at them.
At the top of the World Health Organization’s “critical priority” list sits Acinetobacter baumannii, a gram-negative bacterium that causes devastating hospital-acquired infections — pneumonia, bloodstream infections, wound infections. Carbapenem-resistant strains (CRAB) resist our strongest antibiotics. For patients with CRAB infections in the ICU, mortality rates can exceed 50%.
The standard response is to develop new antibiotics. But new drug development costs over $1 billion and takes 10-15 years. The pipeline is dangerously thin, and bacteria evolve resistance faster than we can innovate.
A Different Approach
What if the answer isn’t a new drug, but a new combination of drugs that already exist?
Drug synergy — where two or more compounds together produce an effect greater than either alone — is well-established in medicine. But the combinatorial space is enormous. With ~60 clinically relevant antibiotics, there are over 1,700 possible pairs and 34,000 possible triples. Testing each one experimentally against even a single resistant strain takes days. Against a panel of clinical isolates? Years.
This is where computational prediction becomes essential.
What We’re Building
At Vibemesh Labs, we’re building a pipeline that combines machine learning with mechanistic reasoning to predict which drug combinations should be synergistic against resistant bacteria — and more importantly, why.
The “why” matters. A statistical model can tell you that Drug A + Drug B scores 0.73 on a synergy metric. But a clinician or grant reviewer needs to understand the mechanism: Which resistance pathway does each drug target? How do they interact at the molecular level? Under what conditions (planktonic vs biofilm growth, iron-limited vs iron-replete media) should you expect synergy?
We produce what we call Mechanistic Causal Dossiers — citation-anchored, step-by-step causal chains explaining the predicted synergy mechanism, along with specific experimental test designs. These aren’t black-box predictions. They’re testable hypotheses with protocols attached.
Why Biofilm Changes Everything
Here’s something most drug combination studies miss: they test bacteria floating freely in liquid (planktonic growth). But in real infections — especially CRAB on ventilator tubes, catheters, and chronic wounds — bacteria live in biofilms. These are structured communities encased in a protective matrix that can make bacteria 100 to 1,000 times more tolerant to antibiotics.
A combination that looks indifferent in a standard lab test might be powerfully synergistic under biofilm conditions, because one drug disrupts the biofilm architecture while the other kills the newly exposed bacteria. Standard checkerboard assays miss this entirely.
Our dossiers specifically address biofilm-mediated resistance and recommend biofilm-condition testing protocols. We believe this is where the most clinically relevant synergies are hiding.
Anti-Virulence: Disarming Instead of Killing
Traditional antibiotic combinations try to overwhelm bacteria with multiple killing mechanisms. We’re exploring a different paradigm: anti-virulence combinations, where one or more drugs don’t try to kill the bacteria directly but instead disable their defense systems — biofilm formation, communication networks (quorum sensing), nutrient acquisition.
Strip away the defenses, and conventional antibiotics that the bacteria had “resisted” can work again. Several FDA-approved drugs have documented anti-virulence properties at sub-therapeutic concentrations, opening the door to repurposing combinations that could reach patients faster than any new drug.
What’s Next
We’re currently seeking academic collaborators with clinical isolate collections and biofilm assay capabilities to experimentally validate our top predictions. If you work on ESKAPE pathogens and are interested in testing AI-predicted drug synergy hypotheses, we’d love to hear from you.
The antibiotics we need might already exist. We just haven’t found the right combinations yet.
This is an ongoing research program at Vibemesh Labs. We’ll be sharing more as results come in. Follow along or get in touch at t.overly@comcast.net.